

Ensign: The Nursing Home Empire Built on Fatal Neglect
Ensign’s business model relies on delivering inadequate care to patients while gaming data on quality, according to a five-month investigation. Patients are dying.

Based on Hunterbrook Media’s reporting, Hunterbrook Capital is short $ENSG and long a basket of comparable securities at the time of publication. Positions may change at any time. This article is not investment advice or a recommendation to buy, sell, or hold any security. Hunterbrook Media is collaborating with organizations like law firms including Hunterbrook Law to pursue reform based on this reporting. See full disclosures on our website.
By: Michelle Cera, Andrew Ford, Laura Wadsten
Editor: Jim Impoco, Sam Koppelman
They beat the walls.
Cheryle Weir couldn’t breathe, her roommate recalled. Dependent on ventilators at an Ensign facility, they couldn’t talk. They couldn’t scream.
So they banged on the table, banged on the wall, desperate for anyone to hear. A nurse should have been there. No one was.
Eventually, Cheryle stopped banging.
Her family’s lawsuit blames her death on The Ensign Group ($ENSG).
Ensign is America’s largest operator of “skilled nursing facilities” (SNFs) — facilities designed to rehabilitate people who need less than hospital care, but more care than they can provide themselves.1
Ensign boasts about its star ratings, “industry-leading” clinical outcomes, and “strong history of quickly improving the quality of care in the facilities we acquire.” A sell-side analyst referred to Ensign’s quality star ratings as part of its “secret sauce.” And Ensign says it sets “the standard by which all others in our industry are measured.”
But a five-month Hunterbrook investigation found that standard is tragically low — and fatal.
The investigation revealed Ensign’s $10 billion empire is built on a dubious foundation: Its profits are heavily dependent on understaffing facilities. It performs better than average on self-reported quality metrics but worse on independently verifiable measures. It regularly violates state minimum staffing laws, and routes taxpayer dollars to its executives and to its own affiliates. Meanwhile, Ensign patients suffer and sometimes die.
“We could’ve had so much more time,” Weir’s daughter, Hanneka White, told Hunterbrook in an interview. “And it was taken away.”

Hunterbrook Media’s reporting team — led by three journalists, as well as former financial analysts from Goldman Sachs and Magnetar Capital — examined millions of Center for Medicare & Medicaid Services (CMS) datapoints, reviewed thousands of pages of documents, and interviewed dozens of sources, including: attorneys, professors, healthcare professionals, ombudsmen, data analysts, and public advocates, as well as former employees of Ensign, residents of Ensign facilities, and family members of Ensign residents.
Here’s the story:
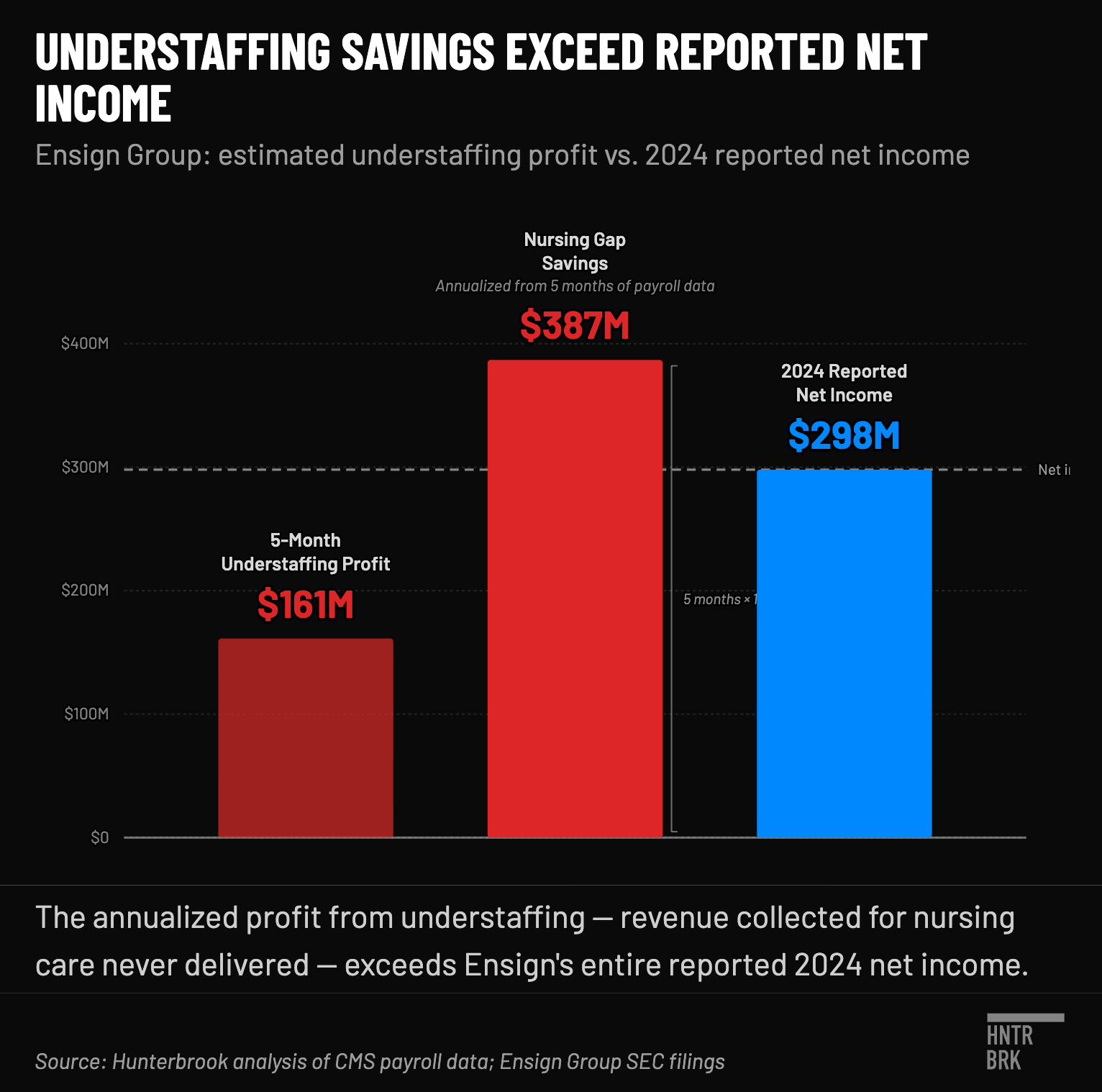
Ensign’s profits can be traced to providing less care than its patients need — and less care than it is meant to provide based on the tax dollars it receives from the government. Government programs pay skilled nursing facilities based on “acuity level,” a measurement of how sick the residents are. Ensign says it’s focusing on high-acuity people in order to increase its revenue, the bulk of which comes from government programs. But then it staffs many facilities below the levels needed to provide the care those payment rates are calibrated to support. Using the formula from a 2025 peer-reviewed study, Hunterbrook calculated a 5 million-hour gap between hours of nursing care needed and hours actually provided at Ensign facilities between July and November 2024, the period for which robust data is available. “The difference between those two numbers is fraud,” opined Ernest Tosh, an attorney who litigates nursing home abuse and neglect cases. Hunterbrook estimates that closing that staffing gap would have cost Ensign about $161 million during the period studied — or roughly $386 million annualized. That’s more than the company’s entire reported net income that year of $298 million. Hunterbrook also found that the more a facility profited from understaffing, the worse its health survey scores, facility-reported incidents, complaint deficiencies, total penalties, staff turnover, and staffing ratings.
The Ensign Effect. We found Ensign’s growth strategy is to buy struggling nursing homes — then cut staff at those facilities and bank the savings, all while claiming quality improves. Ensign has rapidly built its $10 billion empire by rolling up distressed nursing homes, claiming to transform them into “market leaders in clinical quality.” But after Ensign acquires a facility, we found, nursing hours fall. Hunterbrook tracked 161 facilities before and after Ensign acquisition against roughly 15,000 other nursing facilities, controlling for industry trends. Bottom line: The quality of the facilities gets worse, not better, after Ensign acquires them.
Federal and state laws prohibit understaffing. Federal law requires every Medicare- and Medicaid-funded nursing facility to keep “sufficient nursing staff” to meet each resident’s needs. The sicker the resident, the more staffing the law generally demands. Yet Hunterbrook found no consistent relationship between how sick Ensign’s residents are and how many hours it staffs. Four states where Ensign operates impose numeric floors on the care that must be provided: California, Washington, Tennessee, and Kansas. Our analysis of CMS records from 2020 through 2025 found Ensign facilities falling below the legal floors in those states on more than 18,000 days cumulatively. “You have to staff to meet the needs of residents, and that consistently does not happen,” said Ed Dudensing, an elder-abuse attorney, describing insufficient staffing. “That’s illegal.”
Ensign’s superior “star” ratings are largely built on an honor system the company appears to be gaming. The CEO emphasized Ensign facilities “outperformed industry peers in 5-Star Quality Measure results” in a recent press release. He also highlighted “the highest quality clinical outcomes” in an earnings call last year. What he didn’t mention is that those measures are largely self-reported. We sorted CMS Provider Information performance metrics into three tiers: independently verified by unannounced government inspectors; self-reported but auditable via payroll records; or self-assessed and self-reported with no imposed documentation procedures. The result: Ensign performs worse when there is external verification.
Ensign paid more than $339 million to its own affiliates in 2024. That’s about 8% of $ENSG revenue that year. The maneuver is known as tunneling. Our cost-report analysis shows Ensign facilities pay hundreds of millions of dollars a year to entities also owned or controlled by Ensign. Think: Landlords. Insurance. Transportation. “Home office” management fees. Hunterbrook found that, across the industry, more money going to related parties correlates with fewer staffing hours, more staff turnover, and lower health inspection scores, among other metrics. A 2024 congressional letter to Ensign’s then-executive chairman identified the industry practice as a “deceptive tactic” to hide profit. In an interview, Tosh, the attorney, shared his opinion of nursing homes tunneling money to related parties without any effective oversight: “It’s just a huge menagerie of corporations to hide the money movement. In effect it’s money laundering.”
Former employees in different states described systematic misrepresentations. Fabricated Google reviews; document falsification; falls downgraded to “slips;” improperly upcoded patient acuity; and retaliation against staff who refused to engage in these activities. Former employees also told Hunterbrook they were compelled to provide unnecessary care and exaggerate its duration. One former Ensign therapist described higher-ups encouraging higher billing via falsifying minutes of therapy: “The 30 would be erased and somebody would put in a 70.”
An industry lobbying group waged a multi-front campaign to kill a federal government rule meant to stop understaffing. In February of 2026, the Trump Administration rescinded a Biden-era rule setting a federal staffing minimum for nursing facilities, after the American Health Care Association (AHCA), an industry group, sued the government. Ensign and other operators backed a pro-Trump super PAC and Ensign gave $750,000 to MAGA Inc before the rule was rescinded. The now-defunct rule was estimated to save 13,000 lives a year.
Behind all the numbers, patients suffer and die. Thomas Scates died after an Ensign facility neglected him, according to his family. Herbert Howenstein died after a large pressure ulcer developed at an Ensign nursing home. Six inches long, an inch deep, blackened dead flesh, penetrating to muscle. An EMT report shows that facility staff were aware but nobody was treating him for it. An expert reviewing his death concluded, “The patient’s demise was almost merciful.” A nonverbal resident with Alzheimer’s was found covered in ants with bites all over her body — an infestation discovered by her family, not the staff, according to an investigation report. Cheryle Weir died after begging for help that did not come in time, her daughter told Hunterbrook. These are just some of the stories Hunterbrook heard, which represent a fraction of the devastation in Ensign facilities around the country.
Ensign did not respond to multiple detailed requests for comment from Hunterbrook. Ensign CEO Barry Port did, however, tell The Arizona Republic in 2023 that staffing is decided by individual facility management, and the suggestion that his company siphons money to boost profit is “categorically false.” Other statements by the company seem to contradict that supposed distance between Ensign and its individual facilities. In a recent earnings call, for example, Port cited access to patient-level data and involvement in facility-level decisions. The most recent 10-K also suggested there was visibility over individual facilities: Ensign said they use specialized software to help caregivers “more accurately” capture services to “increase reimbursement,” and that the company had “installed software and touch-screen interface systems in each operation.”
To see our full methodology, click here.
If you or a loved one has been affected, or if you have any relevant information to share, please reach out at ideas@hntrbrk.com. This is part one of a series on Ensign and the industry.
“They’re The Model”
Most of us will require institutional care in our lifetime. We hope that care will be high quality.
Faced with an aging population and widespread nursing shortages, every American nursing facility must contend with infections, falls, and sometimes death. On an average day, a facility might smell like human waste cut with cleaning products. Easy listening music covers the croaking sounds of uncomfortable residents. Frontline staff do their best at difficult and low-paying jobs, in facilities lit fluorescently and decorated in liminal beige.
But Ensign has established something worse: a business model that seems to depend on eroding care for America’s sick and elderly.
Our investigation shows the company boomed in recent years by rolling up distressed homes, cutting high-skilled nursing staff, and gaming metrics.
“They’re the model,” said David Kingsley, a retired professor at the Kansas University Medical Center who researches corporations that depend on revenue from Medicare and Medicaid.
Ensign operates the most CMS-certified nursing facilities in America, with 334 locations across 17 states.2 They offer more than 38,000 skilled nursing beds, according to a March filing.
But these facilities have problems — and they seem to get worse after Ensign takes over. Conditions at several of its facilities are so severe that they are candidates on CMS’s “Special Focus Facility” list, a roundup of facilities with a pattern of serious problems that pose risks to resident health and safety. Facilities on the SFF list are at risk of being terminated from Medicare or Medicaid programs.
And Ensign is coming for more. In the second quarter so far, it has announced purchases of 17 facilities in Texas, two in Wisconsin, and one each in Iowa and California (real estate only).
Ensign’s model is working. It grew rapidly after its current CEO took the helm in 2019. His $13.8 million in compensation last year — at a company whose revenue is largely derived from public funds — was mostly tied to company performance.
And Ensign does not limit incentive-based compensation to its senior executives. Our investigation found that some individual facility administrators are compensated the same way, creating powerful incentives to cut costs. While it’s normal to have financial performance incentives for cutting costs, it’s different when the incentive is to cut nursing hours — the results can be a matter of life and death.
For example, a lawsuit deposition shows the company tied a facility administrator’s bonus directly to location profits, and by staffing below recommended levels, that administrator was able to boost a roughly $400,000 annual bonus to more than $800,000.
As a result of understaffing at that very same facility, the lawsuit claims, a resident died, his final moments captured on a recorded phone call provided to Hunterbrook.
One source, a forensic accountant, likened the industry to the Sackler family’s opioid profiteering.
The Multimillion-Dollar Staffing Gap
To mask the sounds of screaming and crying, Doni Hunt Webb plays loud music.
“I know this is neglect and abuse,” she said.
She has lived in an Ensign facility in Utah for more than five years.
“I am a broken person now,” she told Hunterbrook, her voice sounding heavy. “I watch many people in here get broken.”
She described the daily reality of an Ensign facility, which she said was understaffed: persistent hygiene and medical failures.
Hunt Webb said she suffers from extreme nerve damage, a condition she said does not get adequate treatment due to persistent understaffing, turnover, and a lack of training.
At times, staff use wet paper towels in place of toilet paper, Hunt Webb said. She and other residents get recurring infections, she said, recalling that another patient cried and screamed after going a day without food, without being changed, left in a soaking wheelchair.
“The lack of staffing is the number one thing that affects residents’ quality of life,” the deputy state ombudsman in Texas, Alexa Schoeman, told Hunterbrook.
Dozens of studies show this is true.
Public money flows to Ensign and other skilled nursing operators based on the needs of their residents. But many simply don’t staff accordingly.
Each nursing facility funded by Medicare, Medicaid, or both is bound by federal law to have “sufficient nursing staff” to meet the needs of each resident, also referred to as patient “acuity.” The higher the acuity, the more staffing the law generally demands.
And Ensign residents tend to have higher needs than most.
That’s by design, former Ensign employees told Hunterbrook. “They were seeking out people with more complex needs,” said one former therapist. Administrators would deliberately “find the most complex diagnosis of that patient for the highest payback.”
Ensign’s own financial filings indicate their patients are “often high-acuity” and that their “business model is based in part on serving higher acuity patients.” As acuity goes up, so too should hours of care, according to federal law. But Hunterbrook’s analysis found no consistent relationship at Ensign.
CMS commissioned research to time how long it takes to care for residents at different acuity levels. It used this research to set Medicare payment rates, and it informed a federal rule requiring a minimum of 3.48 hours per resident day (HPRD) that was finalized but never put in force before industry lobbying and lawsuits helped convince the Trump administration to rescind it.3
Last year, researchers used those findings to help facilities understand how many nursing hours they need to meet their residents’ acuity — putting a number on the “sufficiency” standard enshrined in federal and state law.
Hunterbrook used this formula and worked with two of the researchers who developed it — Charlene Harrington, professor emerita of UCSF, and Robert McLaughlin, a healthcare data analyst — to calculate the expected number of hours Ensign residents should receive based on the acuity level they report to CMS. Harrington is a leading scholar of nursing home policy, who has spent decades researching the staffing levels needed to ensure safe, quality care.
Next, we calculated the difference between the hours of care patients should receive, based on reported acuity, and the number of hours Ensign actually paid nursing staff to work, according to Ensign’s own filings with the government. In other words, we calculated the gap between what Medicare paid Ensign to provide care and how much Ensign actually spent on nursing staff to deliver that care.
“The difference between those two numbers is fraud,” elder care attorney Tosh said about this gap across the industry.
In 2025, the California Attorney General used a similar technique in a complaint against the nursing home chain Sweetwater. In that case, California analyzed the same CMS database that Hunterbrook used here to allege that the chain systematically failed to meet resident care needs.
Our analysis found Ensign residents were shorted more than 5 million hours in just five months of 2024 — that’s more than 570 years of missing nursing time. The analysis is restricted to this time period due to data availability.
We next sought to translate those hours into dollars, again using Ensign’s own reports on its costs of staffing. We found that Ensign saved about $161 million during those five months by declining to staff its homes adequately. If the trend held across 2024, that’s about $386 million annually in savings on staffing costs, representing profit to the company. For context: That year, Ensign’s entire net income was $298 million.
Across all nursing facilities in CMS data, the profit from understaffing adds up to roughly $6.5 billion across the industry, just from July to November 2024.
Ensign ranks worse than peers: The spread is generally larger at Ensign facilities than the industry norm, according to Hunterbrook’s analysis.
“I think this work breaks ground and is really important because it puts a dollar figure on a staffing question that has been debated for decades,” said McLaughlin, one of the authors of the formula we used in this analysis, who reviewed our work and validated our methodology.
Even these eye-popping figures are likely understated because nursing home operators can inflate the care hours they report to CMS and manipulate their cost reports, according to experts Hunterbrook interviewed.4
With federal rules in flux, some states where Ensign operates have their own minimum staffing laws. A separate Hunterbrook analysis of CMS records suggests Ensign consistently violates the minimum hours-per-resident-day requirements of: California (3.5-hour) , Kansas (1.85-hour), Tennessee (2-hour), and Washington (3.4-hour).5
From 2020 through 2025, in these four states cumulatively, Ensign facilities fell below state minimums on more than 18,000 days.
These minimums represent the lowest staffing level the laws permit.
Ensign regularly fails to meet even that, despite serving residents who are sicker, on average, than those at peer facilities.
When asked directly about our findings regarding the staffing gap and failures to meet minimum staffing levels, Ensign didn’t refute them or offer additional data. The company didn’t respond at all.
There has been some conflicting research on the exact right level — a controversial 2023 study commissioned by CMS declined to recommend a specific minimum HPRD, finding, “no obvious plateau at which quality and safety are maximized.” But there’s good reason for these minimums. That 2023 study still found higher staffing was associated with fewer hospitalizations and emergency room visits.
Understaffing hurts people.
In July 2025, a CMS report shows, a nonverbal resident at an Ensign facility with Alzheimer’s disease was found in her bed covered in ants.
They crawled on her face, neck, legs, and swollen-shut eyes. They left bites all over her body.
Her family said they discovered the infestation — not the staff.
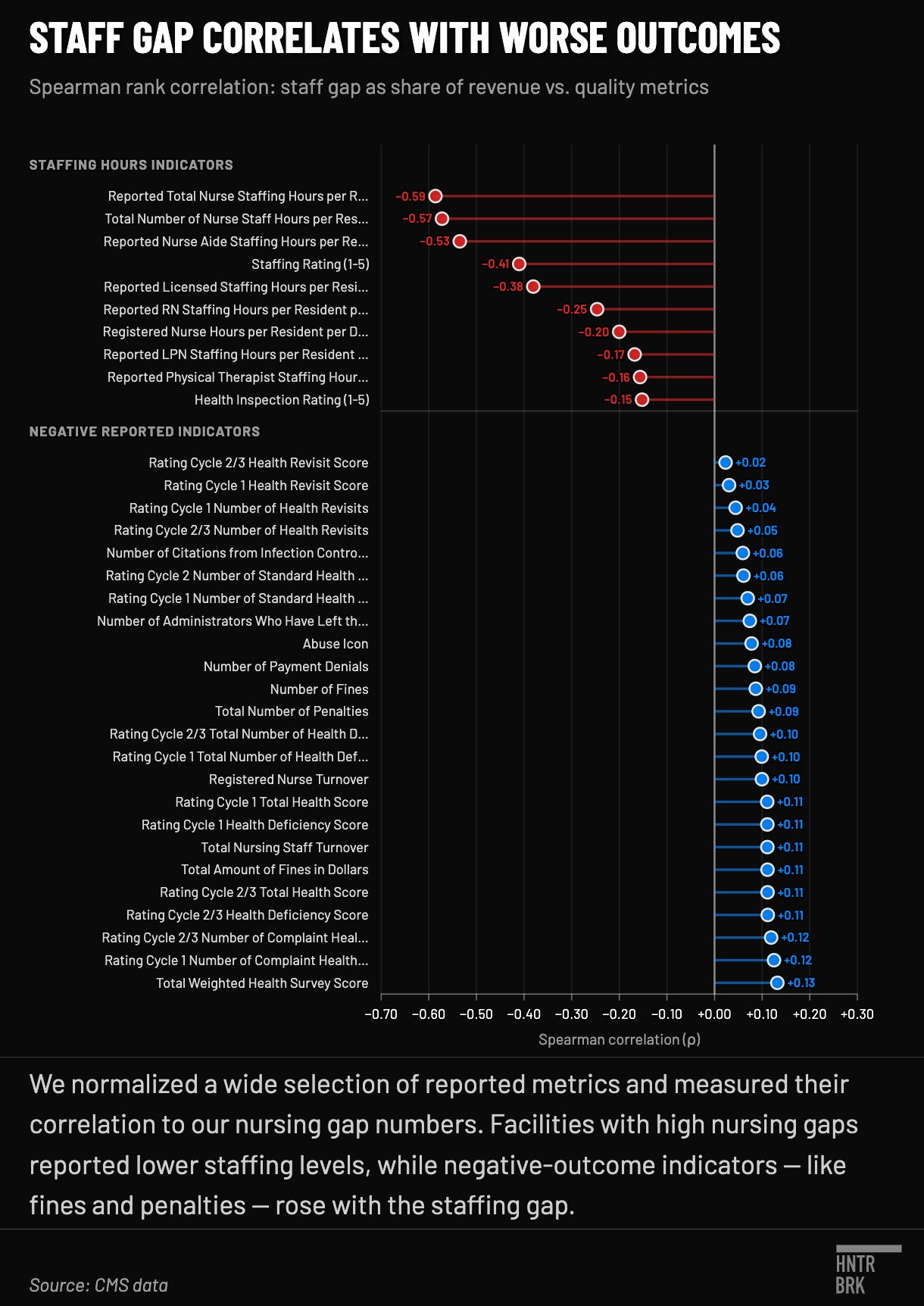
We found a clear pattern across the industry: As spending on staffing decreased, quality metrics deteriorated significantly, including health survey scores, facility-reported incidents, complaint deficiencies, total penalties, staff turnover, and staffing ratings.
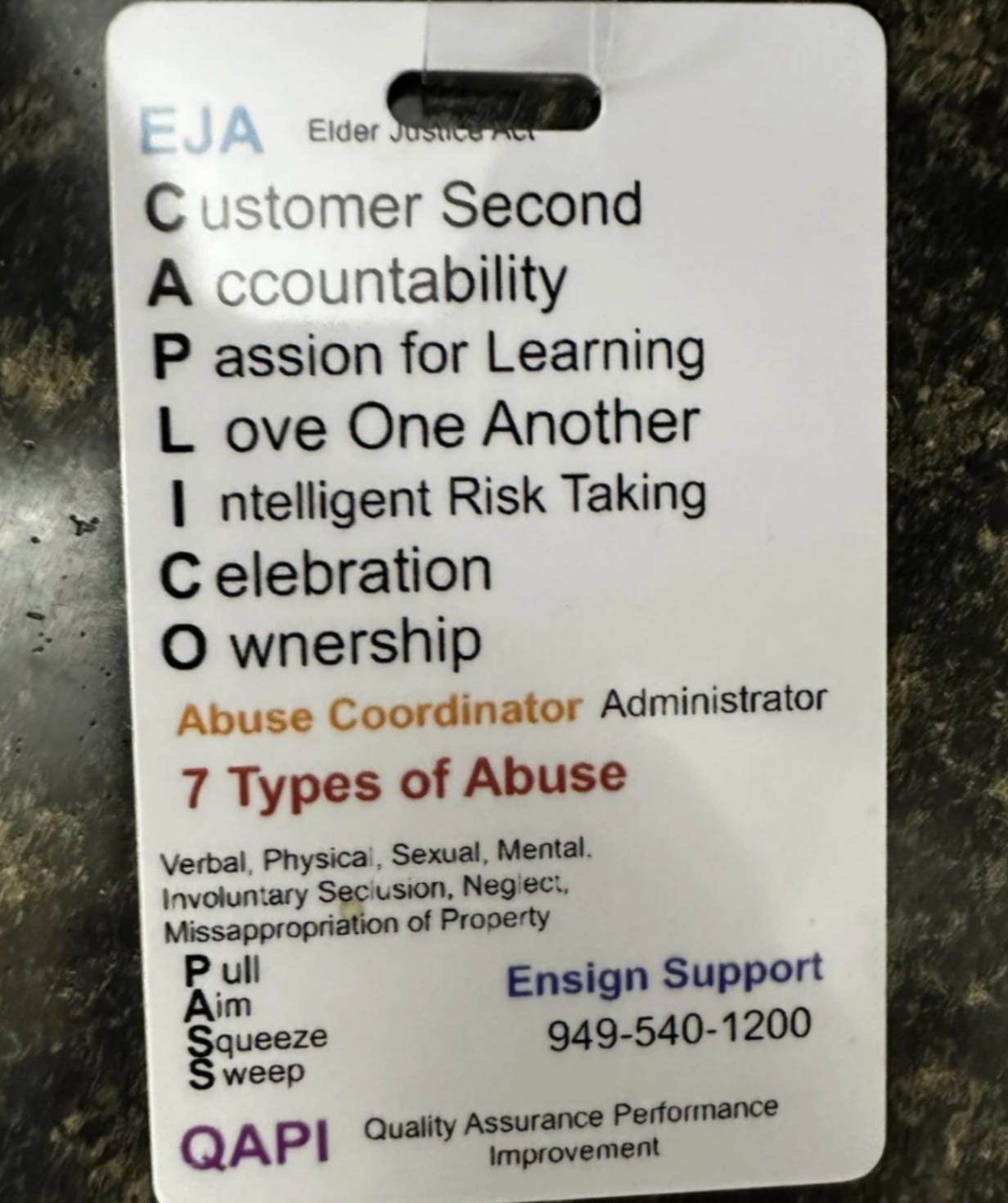
“Customer Second”
Ensign trumpets the acronym CAPLICO across its internal communications, where the first “C” stands for “customer second.” As they explain in the 2026 Code of Conduct, “This means we put our employees first so that they are empowered and inspired to provide the best possible care to our residents/patients.”
A noble thought, perhaps. Yet in interview after interview with Hunterbrook, former employees recounted stories that contradicted Ensign’s purported commitment to its workers.
Robert Love told Hunterbrook that he’d worked as a cook at a Tennessee nursing facility for nine years before Ensign took over. After the sale went through in early 2025, he said, Ensign cut staff.
“You can’t have that mentality in a nursing home setting,” he said of the “customer second” motto. “We have to take care of them.”
Love fed residents grappling with Alzheimer’s disease and dementia. “And to take away resources from that is, I don’t even think that’s bad management. I think that’s just evil greed.”
After Ensign took over, Love said he became one of only two cooks serving roughly 90 residents, his pay was cut, and his hours were slashed. “That’s when I had to go look somewhere else,” he said.
The reduction in pay and hours led Love to take another job cooking fast food at a local gas station, where he made $5 more per hour than his wage at Ensign.
At an Ensign facility in San Antonio, the staffing shortfall was so severe that sometimes nurses would cook for residents, according to a former therapist.
A former physical therapy director for Ensign in Costa Mesa, California, said they were regularly told Ensign could not afford the cost of care.
“We don’t have the means to pay you more, so here, have a pizza party,” they recalled. “It’s kind of become a meme or a joke at this point.”
The data also undermines Ensign’s claimed commitment to its staff. Our analysis showed that when it takes over a facility, Ensign almost invariably cuts staff hours and shifts what hours remain from more skilled, higher paid caregivers to less skilled, cheaper ones.
Again, when asked about these findings, Ensign did not respond to repeated requests.
Staffing levels are not just words on a page or numbers on a spreadsheet — they have real, and sometimes fatal, consequences for Ensign residents.
In 2022, a resident at Ensign’s Clarion Wellness in Iowa was found suspended upside down between a bed rail and headboard, “completely purple and black,” a staff member recalled.
The resident had suffocated.
The facility had installed a grab bar on the resident’s bed without assessing the risk of entrapment, obtaining consent, or evaluating the risks for the resident who had a history of falls, according to findings from Iowa’s State Survey Agency.
Staff didn’t check on the safety of the mattress and bed rails, but a facility maintenance supervisor admitted he marked them as complete anyway. The surveyors also found no evidence that visual wellness checks of the resident were completed.
Iowa regulators condemned the Ensign facility as strongly as they could: They proposed a one-time $10,000 fine.
The same year, Ensign collected more than $8 million in revenue per day.
Self-Reported Metrics Versus Reality: What Happens When No One Is Looking
Over and over, Ensign and its executives swear that they care about patients.
“Our consistent financial results would not be possible without a relentless, patient-focused culture that strives to deliver the highest quality clinical outcomes,” the CEO said in an earnings call last year.
As evidence, the company often cites CMS Star Ratings on quality metrics. For example, in its first-quarter 2026 earnings press release, Ensign’s CEO, Port, touted that facilities “outperformed industry peers in 5-Star Quality Measure results by 24% nationally and 20% at the state level.”
The catch: These ratings are largely based on the honor system, meaning they are self-reported. CMS “does not impose specific documentation procedures on nursing homes,” for most of these metrics, relying instead on expectations of “good clinical practice.”
While higher ratings don’t necessarily mean better quality care, they are likely to matter a lot to an ailing patient or their stressed loved one looking for a nursing facility. The government itself points patients to a website comparing the star ratings of different facilities in order to “compare nursing homes for quality.”
When Hunterbrook first started looking at Ensign’s operations in 2024, there was no obvious reason to doubt Ensign’s quality of care, which appeared high based on its star ratings.
It was only later that we realized that, to a large extent, the quality metrics Ensign likes to cite are largely self-reported and self-assessed.
So, relying on performance metrics documented in CMS Provider Information data for Ensign’s facilities from January 2020 to March 2026, we took a closer look.6
Hunterbrook dove into performance metrics documented in CMS Provider Information data for Ensign’s facilities from January 2020 to March 2026. We separated the various available metrics into three tiers: Tier 1 — Independently verified by state survey agencies contracted by CMS who show up unannounced7; Tier 2 — Self-reported but based on verifiable payroll records and auditable by CMS8; and Tier 3 — Self-assessed and self-reported with no specific documentation procedures.9
We found Ensign outperforms on the metrics the company controls, and underperforms on many of the metrics it has less influence over.
Compared to the national average on Tier 3 ratings, Ensign performed 22% better on the overall quality measure rating, 24% better on long-stays, and 16% better on short-stays — metrics that exist on the honor system. These numbers are unsurprising, given the statistically significant correlation between improved star ratings and profit, documented by multiple studies, and accounts of multiple former employees who said the company underreported adverse events.
The picture looks a lot less rosy for Ensign on Tier 1 and Tier 2 metrics.
On Tier 2 (self-reported but auditable) metrics like registered nurse hours per resident day, Ensign was about 17% worse than the national average. Their staffing rating was 11% worse. And on facility-reported incidents, Ensign performed 38% worse.
Ensign also performed worse on many independently measured metrics (Tier 1): 20% worse on the number of complaint health deficiencies and more than 7% worse on infection control inspections.
Our conclusion: Ensign inflates its grades on metrics it controls, while a truer picture emerges when there is some level of independent verification.
For example, Park Village Healthcare and Rehabilitation in DeSoto, Texas, has five stars on Tier 3 quality measures on the CMS website — a rating that might lead a family or potential resident to think the nursing home is high quality.
The same facility’s one-star (“much below average”) ratings for independently verifiable metrics like health inspections and staffing tell a very different story.
Once more, Ensign did not respond to our questions about its apparent manipulation of the quality rating system.
Misleading ratings can have consequences.
At an Ensign facility in California, a patient had both legs amputated after staff ignored her doctor’s orders to isolate her during chemotherapy, her husband told Hunterbrook. He said the facility placed her in a crowded room next to a resident with pneumonia, and let an infection spiral into sepsis.
The patient’s husband mentioned that they chose the nursing home after reading online reviews and seeing good ratings.
Multiple former employees across different Ensign facilities confirmed for Hunterbrook that ratings were an important internal focus for the company. They described everything from management compelling them to write fake Google reviews to retaliation against employees for not properly manipulating metrics.
“Everything was done on paper,” a former therapist who worked for Ensign told Hunterbrook. A form would go from the facility to building management, who ended up “falsifying before sending it.”
Elizabeth Schlamann, a former certified medical aide for an Ensign nursing facility in Nebraska, told Hunterbrook that corporate directives to their staff were clear: Manipulate the resident assessments that inform star ratings.
“They would literally hold it against us as like a punishment,” Schlamann said, noting that if metrics such as falls and bed sores weren’t manipulated in the way corporate administration wanted them to be, promised perks were withheld.
Staff were also “heavily urged or encouraged” to engage in upcoding, according to Schlamann, a practice where residents are coded as more medically complex than they actually are to increase reimbursement from the government.
Twice when it was scrutinized by regulators, Ensign paid settlements topping $40 million to conclude claims it ripped off the government by billing Medicare for unnecessary treatment and for allegedly paying illegal kickbacks for patient referrals.10
A former speech language pathologist remembered receiving an exit survey before leaving the Ensign nursing home they worked at. The survey asked them if they had seen any unethical behavior or fraud, and promised a follow up call within 24 to 48 hours. They checked yes.
“I didn’t get a phone call,” they said.
The Ensign Effect: Sicker Residents, Fewer Hours of Care
Ensign is known for its aggressive acquisition strategy.
In financial filings, the company attributes much of its historical growth to acquiring SNFs. Ensign’s 2025 10-K claims a “strong history of quickly improving the quality of care in the facilities we acquire.” They point to “consistent improvement” in star ratings post-acquisition as evidence.
In reality, does the quality of care improve in the facilities Ensign acquires?
The data answers with a resounding “No.”
In fact, the analysis revealed what we’re calling “The Ensign Effect.”
When Ensign acquires a facility, the acuity — a measure of how sick residents are — stays higher than the national average, while care provided by higher-skilled registered nurses drops sharply, and total nursing hours go down noticeably too.
“The regulation is that you have to staff to meet the needs of the residents, and that consistently does not happen,” said Ed Dudensing, an elder abuse attorney for 23 years. ”That’s illegal.”
We used 72 months of CMS Provider Information records spanning January 2020 to March 2026 and tracked 161 facilities before and after Ensign acquired them, verified by CMS Change of Ownership records.
We then compared the changes at Ensign facilities to what was happening nationally at roughly 15,000 other facilities over the same time periods, using a technique called difference-in-differences that helps sift the Ensign Effect from broader industry trends.
The result? After Ensign takes over, total nursing hours fall at a statistically significant rate, and continue to fall over time.
The Ensign Effect is especially visible among their higher-paid and most highly skilled employees.
Before acquisition, the registered nurse hours of the facilities hover around the national average. After, a steady decline sets in and widens over the following years.
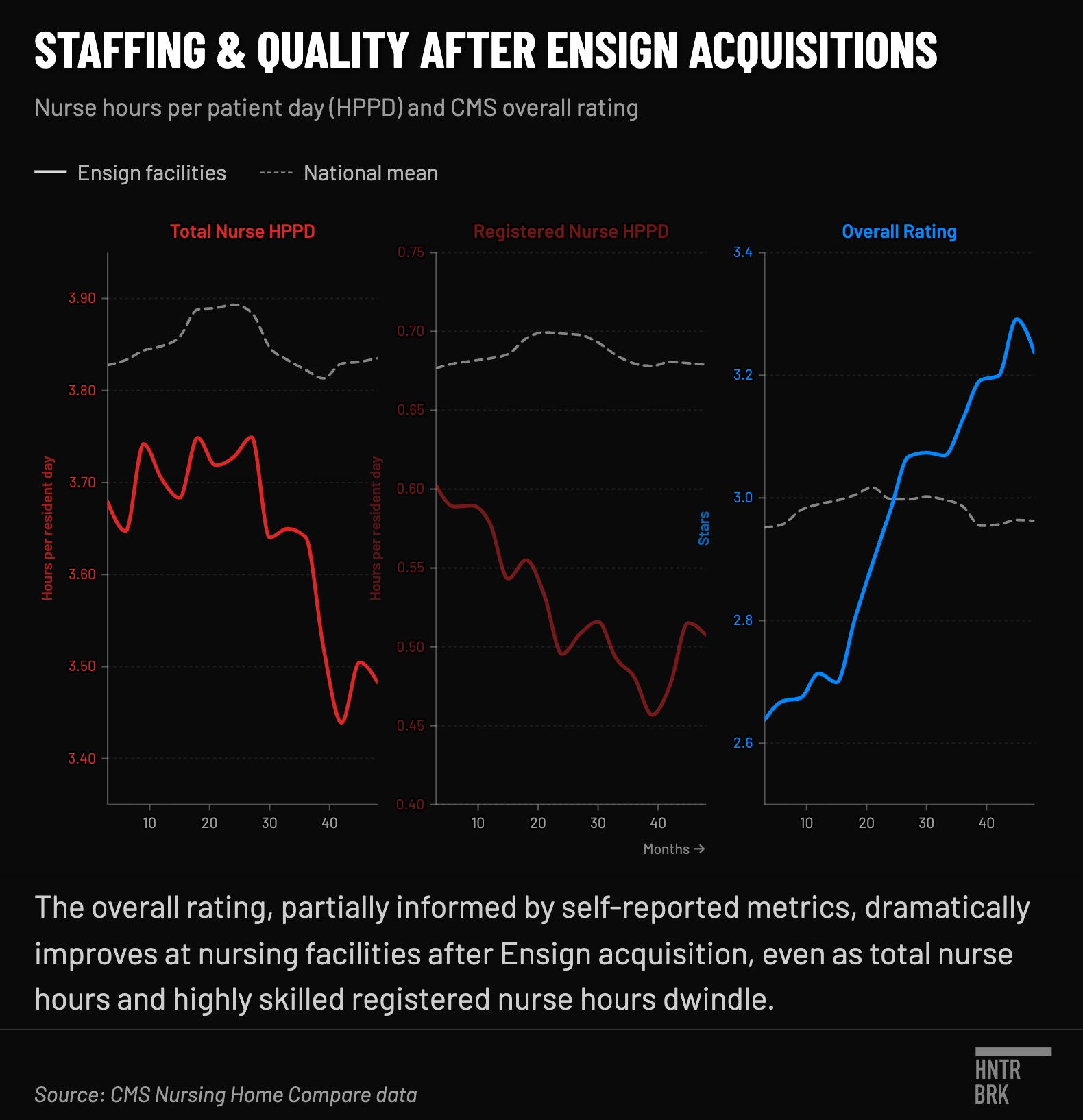
The drop in RN hours also leads to a change in the overall staffing mix.
An increased share of care hours are provided by Certified Nursing Assistants (CNAs) and Licensed Practical Nurses (LPNs), who are less highly trained than RNs and generally cannot provide complex medical assessments or treatments independently.
And yet, while overall nursing care hours and the share of those hours being provided by the most highly skilled professionals is dropping precipitously, somehow Ensign’s overall star ratings consistently improve at facilities it acquires.
How can that be?
Overall ratings — featured prominently on CMS’s Care Compare site where families shop for nursing homes — are built by starting with the health inspection score and then adding up to one star each for staffing and quality measures, including self-reported numbers. Under this methodology, self-reported data can lift a facility’s overall rating by as many as two stars: a 2-star health inspection can become a 4-star overall, and a 3-star can become a 5-star.
Staffing cuts and pushing work onto lower-skilled employees can have serious consequences, according to our sources.
Dominique Haynes, a former CNA at an Ensign facility in Texas, mentioned uncertified staff providing care.
“I constantly saw residents passing away,” she said, referring to the result of dialysis procedures performed by staff she thought were unqualified to do so.
Haynes also described chronic supply shortages. Each morning, she said she went “Easter egg hunting” for scarce supplies. She hoarded wet wipes. Catheters went unchanged, and residents were regularly left sitting in urine.
“They’re scared that they won’t be changed, or that they’re not going to get water, or they’re not going to be taken care of,” Haynes said.
Ensign’s staffing cuts might make sense if the overall patient population at facilities acquired by Ensign also had lower acuity over time. But because the government pays more for higher acuity populations, Ensign actually seeks to acquire facilities where patients are sicker than the national average, Hunterbrook found. Ensign says as much in their public communications, highlighting the sicker-than-average populations in their facilities and telling shareholders that while these struggling nursing homes might negatively affect margins at first, they typically contribute “to earnings within 12 to 18 months.”
The numbers suggest Ensign accomplishes this primarily by cutting down on the staff tasked with the survival of some of the nation’s sickest and most vulnerable people.
But it’s more than just numbers. Reverend Michael Southcombe routinely visited the Pine Crest nursing home in Merrill, Wisconsin. Then he learned the county-owned facility was slated to sell to Ensign. He grew worried about the quality of care under a corporate newcomer.
Driven by a zeal for justice, he became a leader of the grassroots group People for Pine Crest, protesting its sale.
They took their fight to county board meetings, with a self-described “five foot nothing, crippled little old lady,” in fierce opposition.
They got crushed.
The sale went through in 2025, and a group member told a local newspaper that 15 to 20 positions had already been eliminated, employees had their pay cut, and others lost hours.
Nurses are now stretched thin, response time has bloated, and staff that survived the cuts are working harder but getting paid less, Southcombe told Hunterbrook.
“The only way these companies make money is to not provide the care that they’re being paid to provide,” Southcombe said.
Some residents have loved ones who can care for them in the absence of Ensign staff, he added.
“I worry about the ones who are laying there in bed at some end stage of dementia who don’t have family coming to visit them,” Southcombe said.
“Who puts the straw in their mouth when they’re thirsty?”
A Poverty Myth
For years, patient advocates have pointed to understaffing as the single biggest driver of bad clinical outcomes at nursing facilities, and have pushed for regulatory reform in this area. The industry’s main lobbying group aggressively fights any movement toward mandated levels of staffing by claiming they would cause financial ruin.
That group, the American Health Care Association (AHCA), most recently took aim at a federal staffing requirement published in May 2024. It would have required all nursing facilities certified by CMS to provide a minimum of 3.48 nursing hours per resident per day, a level estimated to save 13,000 lives per year. AHCA filed a federal lawsuit the same month, claiming (among other things) that a majority of nursing homes have “negative operating margins” and that the rule would “force them to close their doors for good.”
The AHCA features a rotating cast of characters — and deep ties to Ensign. Ensign’s CEO Barry Port sits on the board of the AHCA, and a former president and CEO of the AHCA, Mark Parkinson, is now on Ensign’s board of directors.
In a 2025 earnings call, Port shared that he had also met with Congressional leadership regarding the staffing minimum. He said it was “to make sure they’re fully educated and understanding of what’s good for funding.”
Around then, Ensign and other major nursing home operators also contributed to a super PAC devoted to President Trump, according to a New York Times report.
And a Federal Election Commission filing showing contributions to MAGA Inc. confirms Ensign donated $750,000 to the president’s super PAC on August 8, 2025.
Continuing their full court press, industry representatives met with the president for lunch at his golf club in the summer of 2025, the Times article said.
By December 2025, the staffing rule was gone.11
Of course, the poverty narrative the industry relied on for its lobbying win is at least somewhat contradicted by the company’s own public statements when talking to another audience: Wall Street.
While AHCA was claiming financial hardship in court filings, Ensign’s CEO was trumpeting “record” and “extraordinary” growth in earnings calls in 2024.
“This plea of poverty when the CEOs are flying around on their private jets is a little hard to bear,” said geriatrician and director of the National Center on Elder Abuse, Dr. Laura Mosqueda.
How Public Funds Become Private Profit
How can Ensign report individual facilities struggling to make ends meet and massive profits at the corporate level?
One answer: A financial arrangement known as “tunneling.”
Here’s how it works: Ensign’s facilities pay separate companies that Ensign also owns or controls for functions like real estate, insurance, and administrative services. Many of these services are necessary to operate the business and each facility would have to pay someone for them. But experts told Hunterbrook that nursing home operators regularly charge themselves excessive, above-market rates when their own affiliates are involved — draining money that could go to staffing while making the facilities appear too financially strapped to provide adequate care.
For the executives at the top, this system works out rather well. Ensign’s CEO took home over $13 million in compensation in 2025. The CFO, almost $12 million. And more than $9 million went to the COO.
More than two-thirds of nursing home profits are tunneled to related parties, a study revised last year found. Another study based on data from 2019 found $1.95 billion in excessive related-party payments across the industry.
“The government is forking over billions of dollars to take care of older and disabled adults,” said Tony Chicotel, an attorney for California Advocates for Nursing Home Reform. “The owners are taking that money and spending the very minimum they can on care.”
A congressional letter sent in 2024 directly to Ensign’s executive chairman at the time, Christopher Christensen, cites these related-party schemes as a “deceptive tactic” the nursing home industry uses to hide profit.
Ensign facilities tunneled about $339 million in total to related parties in 2024, which made up about 8% of the company’s consolidated revenue that year, Hunterbrook found. That’s larger than Ensign’s net income, according to a 2024 financial filing, precisely what the congressional letter warned about.
And this figure is likely understated, given improper reporting to CMS.
“It’s just a huge menagerie of corporations to hide the money movement,” said Tosh. “In effect, it’s money laundering.”
The government prohibits excessive charges, but even when unreasonable costs are caught, CMS doesn’t claw back the money.
And as with understaffing, the data show a consistent pattern: The more nursing facilities pay related parties, the worse their outcomes across some measured dimensions — nurse hours, staffing ratings, turnover, and health inspection scores.
“If we weren’t funding all of this extra expense that comes out of the buildings to all these third parties,” a former Ensign administrator said, “then we would be able to operate and give very, very amazing care to these residents.”
Ensign did not respond to Hunterbrook’s repeated questions regarding its related party transactions.
Riverbend Post Acute Rehabilitation illustrates the dark side of this model.
The 131-bed Ensign nursing home in Kansas City, Kansas, was scarlet-lettered as a “special focus facility” by CMS, meaning it’s among the worst-performing and at risk of losing public funding
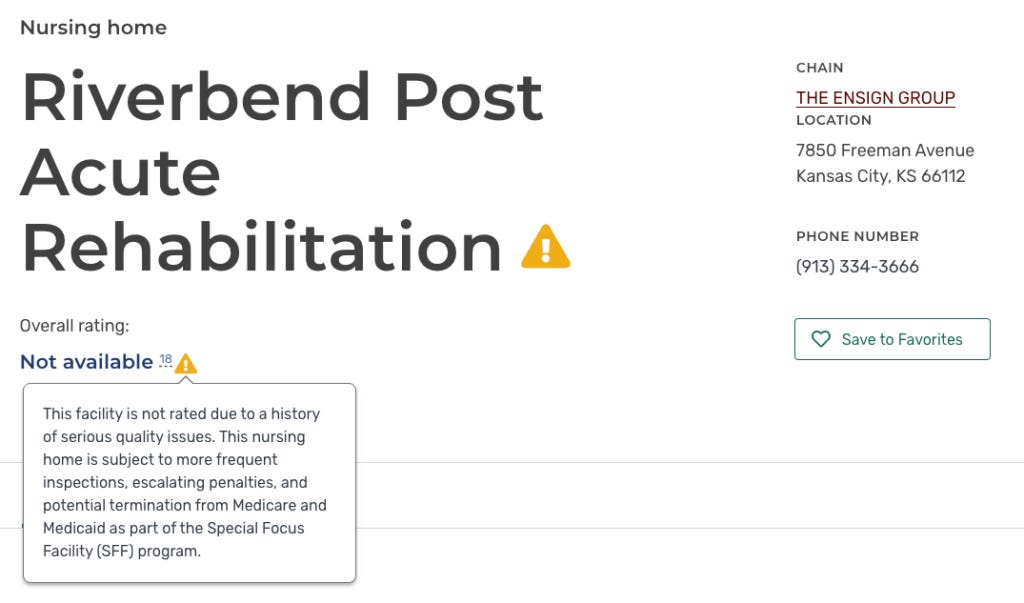
Riverbend is so bad, CMS doesn’t acknowledge it with a rating, but with a warning.
The Ensign facility has been the subject of multiple federal complaint investigations and health inspections. Riverbend was cited for “immediate jeopardy” — the most severe level — after a 2024 investigation found inadequate care led to a maggot infestation inside a resident’s body.
The facility has the money to care for its patients, Hunterbrook found, bringing in nearly $18 million in patient revenue in 2024. But the facility tunnels a massive portion of the money to other Ensign affiliates.
“How do you explain having that much revenue,” Kingsley said, “and yet they can’t take care of a special focus facility?”
Here’s how: In just one year, this nursing home reported more than $2 million in related-party transactions in its cost report to CMS.
Riverbend, meanwhile, has technically lost money in three of the last five years with available data. On paper, it’s barely staying afloat.
But this picture is misleading. Riverbend’s losses are a fraction of the $2 million it sent to Ensign. And this is the crux of the related-party scheme: make the nursing home appear poor on paper while the parent organization extracts its revenue.
In another example of prioritizing profit over care, Riverbend’s cost report shows it relies heavily on lower-cost certified nursing assistants (CNAs) over more expensive and skilled registered nurses.
The theme of replacing more skilled, higher paid workers with lower-skill, lower-cost workers came up twice in interviews with former employees.
A former therapist who worked for Ensign told Hunterbrook they were fired because their position meant they had to be paid more than others.
One former Ensign administrator in training, responsible for tracking expenses, confirmed the pursuit of lower-skilled labor.
“If we can get it cheaper from somewhere else, let’s get it cheaper,” they said, describing their view of Ensign’s mentality. “It doesn’t matter the quality.”
“There’s No Excuse for Killing People”
The dollars on Ensign’s balance sheet are abstractions. But behind them are real people who have been neglected, suffer, and sometimes die in Ensign facilities.
Take the story of Thomas Scates.
Air Force veteran, truck driver, firebrand minister. He thundered in church as he did in cheering his grandson on in football: “I’ll fly away,” he cried from the pulpit, “I’ll fly away.”
When his body started failing, he put his faith in an Ensign nursing facility. Ensign let him fall.
Overburdened nurses didn’t give him enough attention, his daughter, Sharon Thompson, told Hunterbrook. One misdosed his insulin, she said. Then he tumbled out of bed and called for help, but no one came.
“I don’t know how long he was on the floor before somebody showed up,” Thompson recalled.

Ensign staff just put him back in bed, Thompson said. The Scates family filed a lawsuit, later dismissed on technical grounds rather than the merits of the case, claiming he died because Ensign’s facility in Peoria, Arizona neglected him.
“They did not take him to the hospital,” Thompson added. “They did not call a paramedic.”
The family’s complaint claimed Scates’ injuries were preventable, yet the facility was chronically understaffed and undertrained in an effort to maximize profit.
Scates’ experience seems to reflect patterns Hunterbrook found across Ensign’s facilities. Our analysis concluded that Ensign has turned the suffering and neglect of the nation’s most vulnerable into a lucrative business model: seeking out medically complex residents to extract as much revenue as possible, siphoning hundreds of millions of dollars to Ensign’s own affiliates, pocketing vast sums by staffing below the level their residents need, and showcasing self-reported quality metrics to investors and the public.
The ethical conclusion is simple in the eyes of a professor widely known for her research and advocacy in this area, Charlene Harrington.
“When you have a multibillion-dollar corporation,” Harrington said, “There’s no excuse for killing people.”
If you or a loved one has been affected, or if you have any relevant information to share, please reach out at ideas@hntrbrk.com. This is part one of a series on Ensign and the industry.
Authors
Michelle Cera trained as a sociologist specializing in digital ethnography and pedagogy. She completed her PhD in Sociology at New York University, building on her Bachelor of Arts degree with Highest Honors from the University of California, Berkeley. She has also served as a Workshop Coordinator at NYU’s Anthropology and Sociology Departments, fostering interdisciplinary collaboration and innovative research methodologies.
Andrew Ford is an investigative journalist who exposed systemic flaws and prompted reforms in healthcare, business, policing and state government. His reporting was published by ProPublica, USA Today, The Arizona Republic, Asbury Park Press, and Florida Today. He holds a journalism bachelor’s from the University of Florida and received a data analytics master’s from Georgia Institute of Technology. He taught data journalism to investigative journalism master’s students at the Walter Cronkite School of Journalism and Mass Communication at Arizona State University. Andrew is based in Phoenix, Arizona.
Laura Wadsten is an investigative journalist specializing in healthcare. She began her career reporting on antitrust and health care markets as a Correspondent for The Capitol Forum, a premium subscription financial publication. Previously, she was Executive Director of the nonprofit Moving to Value Alliance, where she produced the MTVA Unscripted Podcast. Laura was a Hodson Scholar and Editor-in-Chief of The News-Letter at Johns Hopkins University, where she earned a B.A. in Medicine, Science & the Humanities.
Editors
Jim Impoco is the award-winning former editor-in-chief of Newsweek who returned the publication to print in 2014. Before that, he was executive editor at Thomson Reuters Digital, Sunday Business Editor at The New York Times, and Assistant Managing Editor at Fortune. Jim, who started his journalism career as a Tokyo-based reporter for The Associated Press and U.S. News & World Report, has a Master’s in Chinese and Japanese History from the University of California at Berkeley.
Hunterbrook Media publishes investigative and global reporting — with no ads or paywalls. When articles do not include Material Non-Public Information (MNPI), or “insider info,” they may be provided to our affiliate Hunterbrook Capital, an investment firm which may take financial positions based on our reporting. Subscribe here. Learn more here.
Please contact ideas@hntrbrk.com to share ideas, talent@hntrbrk.com for work opportunities, and press@hntrbrk.com for media inquiries.
LEGAL DISCLAIMER
© 2026 Hunterbrook Media LLC. When using this website, you acknowledge and accept that such usage is solely at your own discretion and risk.
Hunterbrook Media LLC (”Hunterbrook Media”) is an investigative news organization. Hunterbrook Media is affiliated with Hunterbrook Capital LP (”Hunterbrook Capital”), an exempt reporting adviser with the U.S. Securities and Exchange Commission that serves as investment adviser to one or more investment funds. Hunterbrook Media and Hunterbrook Capital are legally separate entities under common control. Hunterbrook Capital’s investment activities support Hunterbrook Media’s journalistic operations. Hunterbrook Capital’s investment performance can be affected by price movements in securities, derivatives, or other financial instruments related to companies covered in Hunterbrook Media’s reporting.
The specific position, if any, held by Hunterbrook Capital at the time of publication is disclosed at the top of this article. Any position or exposure may consist of direct holdings, short sales, options, swaps, other derivatives, or other forms of economic exposure to the securities or issuers discussed herein. Any position held may include equity securities, options, swaps, or other derivative instruments. Consistent with applicable policies and procedures, Hunterbrook Capital may establish, modify, or close positions in covered securities before or after this article is published. Following publication, Hunterbrook Capital will continue transacting in covered securities for an indefinite period and may hold long, short, or no positions at any time thereafter, regardless of any position described at publication. Hunterbrook Media has no obligation to update this article to reflect subsequent changes in Hunterbrook Capital’s positions. Any discussion in this article regarding value, valuation, downside, upside, or potential future stock price reflects Hunterbrook Media’s opinion as of the publication date. Such statements should not be interpreted as price targets and should not be understood to mean that Hunterbrook Capital intends to maintain any position until any particular price, valuation, or outcome is achieved. Hunterbrook Capital may modify, reduce, increase, hedge, or close positions at any time for risk management, portfolio management, liquidity, regulatory, investor, or other business reasons.
Nothing herein constitutes investment advice, a recommendation to buy, hold, or sell any security, or a solicitation to purchase or sell any securities. Hunterbrook Media is not a registered investment adviser in the United States or any other jurisdiction. All information and opinions presented are subject to change without notice.
Hunterbrook Media strives to ensure the accuracy and reliability of the information provided, drawing on sources believed to be trustworthy. Nevertheless, this information is provided “as is” without any guarantee of accuracy, timeliness, completeness, or fitness for any particular purpose. Hunterbrook Media does not guarantee the results obtained from the use of this information, and expressly disclaims any warranty, express or implied, as to accuracy or reliability. You should conduct your own research and seek advice from qualified financial, legal, and tax professionals before making any investment decisions based on information obtained from Hunterbrook Media.
The content provided by Hunterbrook Media does not constitute an offer to sell, nor a solicitation of an offer to purchase, any securities. No securities shall be offered or sold in any jurisdiction where such activities would be contrary to applicable securities laws. Hunterbrook Media authorizes redistribution of these materials, in whole or in part, for non-commercial, informational purposes only, provided that such redistribution includes this notice without alteration. Commercial use or alteration of these materials requires the express written approval of Hunterbrook Media LLC. By accessing this content, you agree to Hunterbrook Media’s Terms of Use.
According to April 2026 CMS data, The Ensign Group operates 334 CMS-certified nursing facilities across 17 states — larger than the market capitalization of its competitors PACS, National Healthcare Corporation, and Brookdale Senior Living. Ensign operates several types of nursing facilities, but we focus on their facilities that are CMS-certified, the vast majority of which are SNFs, and SNFs account for over 95% of Ensign’s revenue.
Figures are from the April 2026 CMS archived data snapshot for “nursing homes including rehab services.” They may be incomplete.
The HPRD requirement was eliminated in two steps: 1) a federal court vacated the provision in April 2025, the Trump administration initially appealed but abandoned the appeal in September 2025; and 2) CMS then formally rescinded it by interim final rule in December 2025. The court did not question the validity of the 3.48 HPRD figure itself or the research behind it; it vacated the rule because CMS declared the standard would be “implemented and enforced independent of a facility's case-mix,” which contradicted Congress's requirement that staffing be “sufficient to meet the nursing needs of its residents.”
A 2024 report by the Department of Health and Human Services Office of Inspector General also found that some nursing homes failed to accurately report related-party costs.
California offers a waiver of the 3.5 HPRD minimum for workforce shortages, but a lawyer for California Advocates for Nursing Home Reform told Hunterbrook the waiver is “rarely granted.” We are not aware of equivalent waivers in Kansas, Tennessee, nor Washington.
This analysis accounted for Ensign’s acquisitions from February 2016 to March 2026 through CMS’s Change of Ownership dataset, and only included facilities previously owned by Ensign or newly acquired facilities. The analysis also includes a 12-month buffer period to exclude prior operators’ performance data because CMS conducts health inspections roughly once a year.
We organized the three tiers in this analysis according to how CMS describes the metrics it uses. Tier 1 metrics are generated by independent state survey agencies conducting unannounced inspections under contract with CMS. The Five-Star Technical Users’ Guide confirms that health inspection ratings are based on the “number, scope, and severity of deficiencies identified during the two most recent annual inspection surveys, as well as findings from the most recent 36 months of complaint investigations and focused infection control surveys” — meaning total deficiency counts, standard survey deficiencies, complaint investigation deficiencies, and infection control citations originate from what state surveyors document on-site. The abuse icon is triggered by harm-level citations found during surveys. No Tier 1 metric relies on facility self-reporting.
Tier 2 metrics — staffing ratings, reported nurse aide hours per resident day, RN hours, LPN hours, total nursing hours, nurse hours on the weekend, and turnover rates — are derived from Payroll-Based Journal (PBJ) submissions, which Section 6106 of the Affordable Care Act requires to be "based on payroll and other auditable data." While facilities self-report this data, it is anchored to payroll records that can be independently audited, and since October 2022 CMS has directed state surveyors to use PBJ staffing data during inspections. The number of facility-reported incidents is self-reported by facilities but is included in Tier 2 because federal regulations require skilled nursing facilities to report these incidents to state survey agencies, who then investigate and may conduct on-site surveys in response (State Operations Manual, Chapter 5).
Tier 3 metrics — the overall quality measure rating and the long-stay and short-stay QM ratings — are calculated largely from MDS assessments that the facility completes and submits. The MDS 3.0 Quality Measures User's Manual confirms that quality measures are calculated using MDS data, which is self-reported by the nursing homes.
If Ensign has continued these behaviors, then some percent of the apparent understaffing in the data may actually be due to upcoding, which can also be illegal.
In 2024, CMS published a final rule setting a minimum 3.48 hours-per-resident-day (HPRD) total nurse staffing requirement and a 24/7 onsite RN requirement, to be phased in over several years. The 3.48 HPRD floor and the 24/7 RN requirement were scheduled to take effect for non-rural facilities on May 11, 2026, and for rural facilities on May 10, 2027. They never took effect. CMS issued an interim final rule in December 2025 rescinding the HPRD and 24/7 RN provisions, effective February 2, 2026 — roughly three months before the 3.48 HPRD and 24/7 RN requirements would have first applied to non-rural facilities. Congress also enacted a moratorium on enforcing the HPRD and 24/7 RN requirements until 2034, in Section 71111 of the One Big Beautiful Bill Act.